A Communication Problem
The invention that solved one of cardiology's oldest problems

In 1944, in the midst of World War II, Dwight Harken, an American surgeon deployed to the UK, was tasked with setting up a chest surgical center as part of the 160th General Hospital in rural Gloucestershire, England. The goal was to begin to perform heart surgery on wounded soldiers. At the time, performing surgery on the heart was genuinely unprecedented — patients rarely survived this procedure. However, the numbers of soldiers arriving with embedded shrapnel, bullets, and shell fragments in their hearts made the decision to try this acceptable. And the fact that Harken had successfully performed similar procedures on animals made him the logical candidate to set up the center. Harken was joined by Paul Zoll, a Harvard-trained cardiologist and researcher, who was deployed to England and served as Chief of Medicine at the same hospital. He supported Harken during the surgeries, and the pair removed shrapnel and bullets from in and around the hearts of 138 soldiers, without a single fatality.
Zoll had observed that the hearts of the wounded soldiers contracted with the slightest stimulus during surgery — an observation that stayed with him when he returned from the war. In 1947, a patient under Zoll’s care, who was experiencing fainting spells from an intermittently stopping heart, died. An autopsy revealed that the heart itself was not structurally damaged. The muscle was healthy, there was no coronary disease or other damage — the problem was a faulty electrical system. In a healthy heart, the muscle contracts only after it receives an electrical signal from the sinoatrial node, a cluster of cells in the upper right chamber that sends the signal to the lower chambers, which actually pump the blood. In the case of Zoll’s patient, that signal never arrived. Pairing this insight with what he saw in the surgical center with Harken — that the heart responded to stimulation — Zoll set out to show that a broken internal electrical signal in the heart could be replicated by an external device.
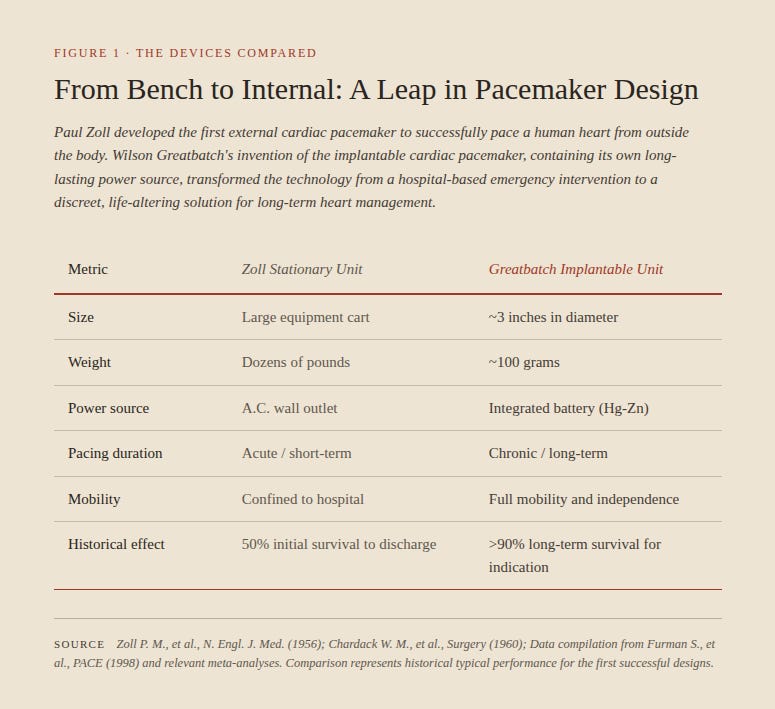
Zoll spent the next several years building his device, testing it on animal models, and eventually moved to a test on a 65 year-old man with end-stage coronary disease and complete heart block — meaning no electrical signal was passing from the upper to the lower chambers of the heart. The external stimulation was successful for 52 hours, and the patient survived for 6 months. He published his results in November 1952 in the New England Journal of Medicine.1
However, the machine was very hard on the patients — it was painful, immobilizing, dependent on a wall socket, and left burns on the skin — very far from ideal. A new approach was needed to produce a device that was both functional and easier on the patients, and that would arrive because of a fortuitous misstep.
Working at Cornell’s animal behavior farm, Wilson Greatbatch was building an oscillator to record heart sounds when he inadvertently placed the wrong resistor into the oscillator. When he turned it on, the circuit began pulsing for 1.8 milliseconds, then stopped for one second and then repeated. Greatbatch recognized that this rhythm mirrored that of a heartbeat — and he decided to quit his job and dedicate himself to building this device. In 1958, he used the $2000 he had saved, set up shop in the barn behind his house, and proceeded to build 50 prototype pacemakers by hand. He spent the next two years working with Dr. William Chardack and Dr. Andrew Gage who performed pre-clinical work on dogs. In June 1960, at a hospital in Buffalo, Chardack implanted a Greatbatch pacemaker in a 77 year-old man with complete heart block. The patient survived another 18 months, and that same year nine other patients received the implant, with two of the original 10 living for another 20 years. Also in 1960, Greatbatch and Medtronic entered into a 10 year licensing deal to manufacture the pacemakers, though Greatbatch retained complete control over all design elements for the entire period. Within a few years, over 10,000 pacemakers had been implanted globally. But there were challenges with these early versions — notably, the life of the batteries. And Greatbatch continued to work on a solution to this.
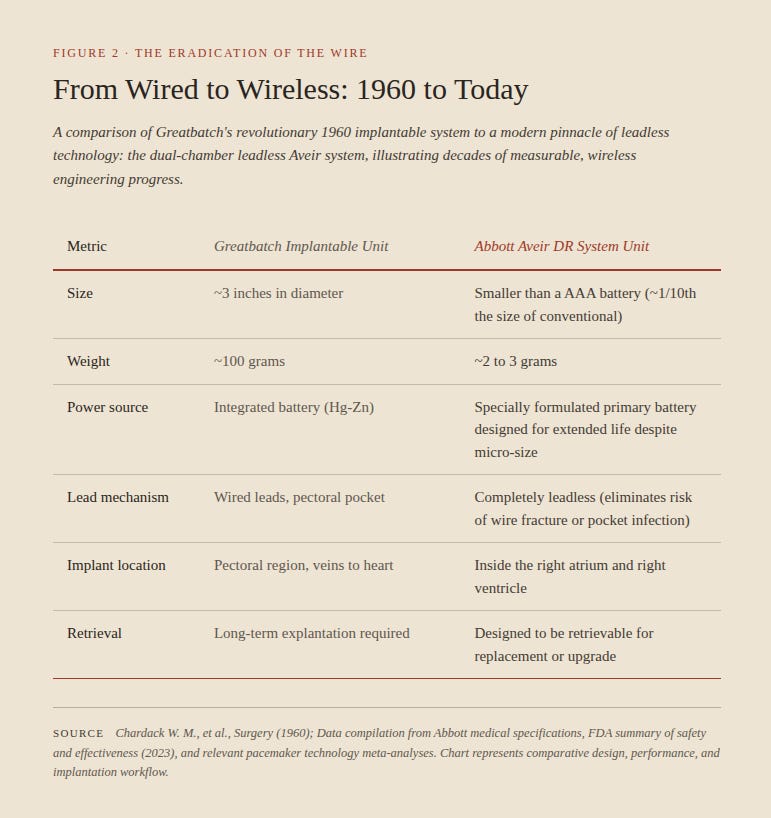
Mercury-zinc was the original battery used in Greatbatch’s pacemaker, and this remained the case for the next 15 years. The lifespan of these was only two to three years — meaning, when they failed, another invasive procedure was required to replace it. Given that most patients receiving these were in their seventies, this was an obvious problem. In 1968, Greatbatch acquired the rights to a lithium-iodine battery from a Baltimore-based company called Catalyst Research Corporation. He reengineered this into a compact battery suitable for implantation into a human body, and began to manufacture them under his newly formed company Wilson Greatbatch Ltd. By 1972, they began to be used in pacemakers, and remain the standard today — and with a lifespan of 10 years. By 1978, only 5% of implants were using the old mercury-zinc batteries, and by 1981 there were 500,000 Americans living with pacemakers.2
Most of the developments over the past decades have focused on improving pacemaker functionality, but the basic system — a pulse generator connected to leads threaded through veins and into the heart — remained largely the same. This changed in 2016, with the introduction of leadless pacemakers, which eliminate the complications that can be caused by the leads. They are the size of a large vitamin capsule, and are inserted through the femoral vein in the leg, and implanted via a catheter directly into the heart’s right ventricle. More recently, Abbott Labs received FDA approval in 2023 for a system with two separate devices, one each for the upper and lower chambers, which coordinate wirelessly and can serve a broader group of patients.
Greatbatch’s two key innovations — implantability and a 10-year battery — turned a two-year medical procedure into a 10-year solution. Today, up to 3 million Americans live with pacemakers, according to Yale Medicine. The majority of the patients are 65 and older, and the aging baby boomer population means the demand for these will likely grow in the coming decades. Before Zoll connected what he witnessed in England with the death of one of his patients, a complete heart block was a death sentence. It was a communication problem between two sections of the heart, a problem that has now been solved for millions.