Turning the Tide on C. diff
The long, multi-front response to one of medicine's most stubborn infections.

In 1958, Ben Eiseman, the Chief of Surgery at Denver General Hospital, and his colleagues were treating patients with severe inflammation of the colon that they could recognize on sight but could not attribute to a specific cause. Eiseman had a hunch that the disease they were seeing was caused by a disruption in the normal bacteria of the gut related to antibiotic use by the patients. They performed an intervention with four patients, three of whom were severely ill, treating them with enemas of healthy human stool — taken from healthy patients. Eiseman’s hypothesis at the time was that introducing healthy donor bacteria into the patients would allow the protective microbial community in the gut to re-establish and heal itself. All four of the patients recovered.1
At the time of Eiseman’s intervention in 1958, the disease they were treating was not widespread — but the fatality rate was acute — estimated to be as high as 75%. That same year, the FDA approved a new antibiotic, vancomycin, developed in part to treat strains of staph infection in hospitals that had become resistant to penicillin. It turned out that vancomycin was an effective treatment for the disease Eiseman had treated — and was much-preferred by physicians — compared with the unconventional procedure used by Eiseman. It quickly became widely used to treat the disease. While vancomycin cleared the infection, the mechanism was not understood. It would be twenty years before the cause was uncovered — and it was a different antibiotic that would lead scientists there.
Clindamycin, a broad-spectrum antibiotic, was approved by the FDA in 1970 to treat a range of infections — and over the next few years it was widely prescribed. Clinicians began to notice that its usage was frequently associated with a severe form of colitis — which they termed clindamycin colitis. In this case the antibiotic was not the cure — rather, it was a contributing factor to the spread of the disease. By the mid-1970s, the growing number of cases prompted scientists to seriously investigate the root cause. Researchers at Tufts University traced the disease to a toxin-producing bacterium, Clostridioides difficile — shortened to C. diff — and at the same time the researchers showed that vancomycin was actually attacking C. diff directly.
Because of the effectiveness of vancomycin, a continuation of the treatment that Eiseman had successfully performed became a secondary priority. While a few physicians continued to build on Eiseman’s work, it was largely out of the mainstream. For the next 15 years, C. diff became a somewhat manageable problem — it was primarily limited to hospitalized patients on antibiotics. Vancomycin and another recently approved antibiotic, metronidazole, were successful in treating infected patients, and hospitals tightened infection control practices to limit the spread of C. diff. However, during the 1990s it became clear that this was not a sustainable solution.
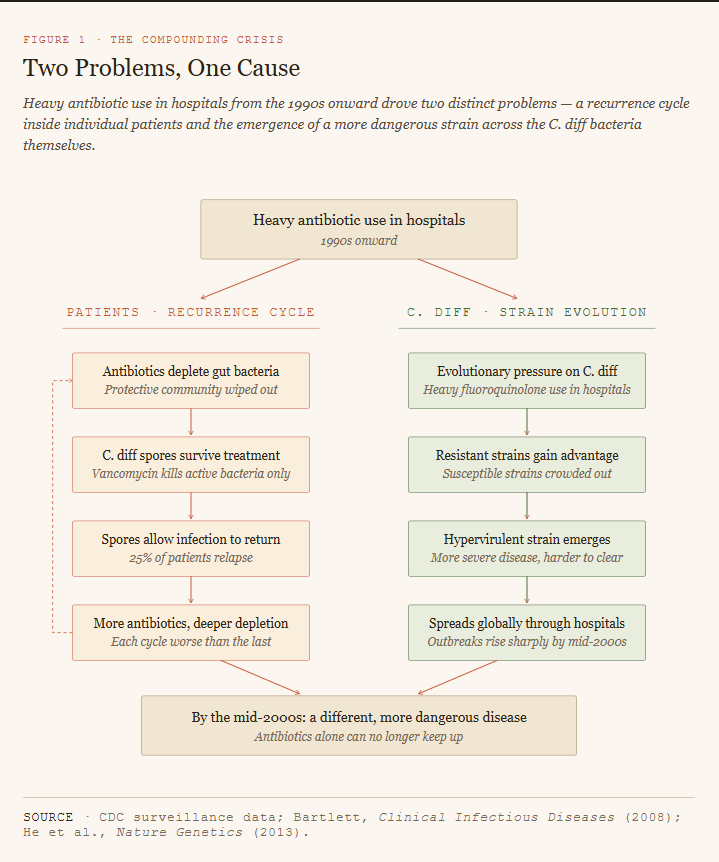
Widespread use of new broad-spectrum antibiotics through the 1990s and into the early 2000s — in particular fluoroquinolones — created a problem for the standard treatment protocol. While these new antibiotics were effective at treating a range of bacterial diseases, they also wiped out the protective bacteria in the gut that prevented C. diff from taking hold. C. diff forms hardy spores that survive vancomycin treatment and can persist in the gut for weeks — so with the protective bacteria depleted by these new antibiotics, C. diff has an easier time getting re-established in the gut. The result was that many patients who were treated with vancomycin faced a relapse — by the mid 1990s, about 25% of patients faced recurrence of C. diff, and the number of multiple recurrences was growing. With each recurrence and subsequent treatment, the next recurrence was more likely, creating what physicians termed a “recurrence cycle.” In addition to the recurrence problem in patients, the C. diff bacteria were also evolving resistance to fluoroquinolones, which made antibiotics alone insufficient to address the recurrence cycle. So these two distinct problems — patient recurrence and C. diff antibiotic resistance — compounded each other, and could both be traced back to heavy use of antibiotics in hospitals. It was obvious that antibiotics alone were not going to address this crisis.
Meanwhile, a physician from Australia, Thomas Borody, was working to refine the process first used by Ben Eiseman — focusing on restoring the ecosystem in the gut, rather than using an antibiotic to kill the pathogen. Borody developed a series of protocols to help standardize the process, and treated hundreds of patients with a reported success rate of about 90%. As the problems with recurrence from heavy antibiotic use continued to grow through the 1990s and 2000s, the medical establishment began to recognize Borody’s approach — what was later termed fecal microbiota transplantation (FMT) by the medical community — as a way to break the recurrence cycle that antibiotics alone could not.
In January 2013, the New England Journal of Medicine published the results from a publicly-funded small randomized trial of more than 40 patients who had previously been treated for C. diff, but had experienced a recurrence. Led by Els van Nood, a physician at the Academic Medical Center, University of Amsterdam, the patients participating in the trial were divided between those receiving FMT (16) and those receiving vancomycin (26). The results were so stunning that the safety monitoring board stopped the trial before it was completed — 81% of patients from the FMT arm were cured after a single infusion, compared with only 31% from the vancomycin arm. The safety board determined that continuing to enroll patients in the non-FMT arm of the trial when a clearly superior treatment was available was not ethically justified. Over the next few years, a number of subsequent studies from researchers in the US, Canada, and Italy confirmed the van Nood results. It was clear by this point that FMT had an important role to play in the treatment of C. diff.
In the early 2020s, the FDA approved two new medicines, both standardized forms of FMT, that were focused on addressing the recurrence cycle. Antibiotics such as vancomycin remain the first line treatment for new cases of C. diff — while both of these new medicines interrupt the recurrence problem by building back the healthy bacterial community in the gut. Rebyota, approved in late 2022, is administered as a single-dose enema by a health care provider. By contrast, Vowst, approved in early 2023, is an oral capsule, removing the need for patients to travel to a healthcare facility for treatment. While these products are still relatively new, and the cost is very high, both of these medicines have made the delivery of FMT as a therapy more accessible to more patients. And the cumulative effect of all of this — antibiotics, infection control, FMT, and now these new drugs — has been positive and measurable.
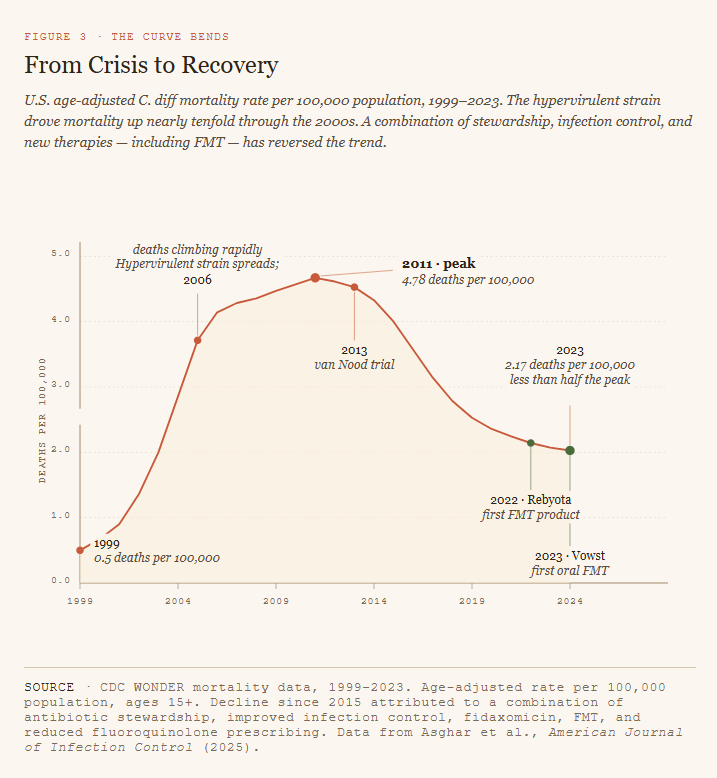
It has been almost seven decades since Eiseman conducted his pioneering test of FMT and ushered in a new way of treating a then-rare but devastating disease of the gut and colon. The path to the current approach has been complicated and bumpy. Identifying the cause was the first major hurdle, and vancomycin proved successful in treating this. Later, as new antibiotics were introduced to treat specific diseases — and were successful in doing so — they unexpectedly created a crisis in C. diff, leading to a renewed interest in the Eiseman approach. It turns out a healthy bacterial community in the gut, the focus of FMT, is a primary contributing factor to staving off C. diff. The path was not smooth at all times, but eventually the collaborative efforts of the research community, regulators, and health care providers began to turn the tide. The mortality curve, after climbing through the 2000s and peaking in 2011, has for the past decade been trending downward and has now been reduced to less than half the peak.
References:
1 https://pmc.ncbi.nlm.nih.gov/articles/PMC4030611/